I had the opportunity to interview Dr. Danielle Levac, Associate Professor at the Université de Montreal in the School of Rehabilitation Sciences. Her research is innovative, exciting and focuses on an emerging biomedical technology, making her the perfect person for this interview.
Dr. Levac joined UdeM just over a year ago, where she continues to explore the research program she began at Northeastern University in Boston in 2015. She leads the “Laboratoire d’Innovations Numériques, Polytechniques et Interactives en Réadaptation pour Enfants” (LaboINSPIRE) which looks at integrating digital innovations like virtual reality and video games into rehabilitation for children and youth with disabilities. Her current research projects revolve around 3 big areas:
- How to use and measure the effects of digital technologies in rehabilitation?
- How do these virtual environments affect learning and do the skills acquired during virtual interventions transfer to the real world?
- How to support clinicians to integrate these digital tools into clinical practice?
I began by getting to know more about her background as a physiotherapist and what lead her to her current research interests:
What motivated you to go into physiotherapy?
“I was exposed to a lot of physiotherapy as a child due to an orthopedic condition that I had growing up, so I was always in physiotherapy. I think for me, I liked the idea of the scientific aspect but also the interpersonal aspect. I saw how not only was it important to have an understanding of movement but how that body is in context of its environment, interpersonal relationships and all the factors that can influence how a person moves. For me, physiotherapy was the choice to combine my interest in medicine and health but also wanting to develop relationships and have a real-world impact.”
What inspired you to pursue research in this field?
“After several years as a physiotherapist, always in pediatrics, I knew there was always questions you don’t have the answers to. For me to have always enjoyed self-directed learning and the academic atmosphere, it made sense to combine my clinical work with a Master’s and then PhD. I really enjoy the academic environment and wanted to teach other students to stay involved clinically but also to advance the field of physiotherapy, which although there is a great deal of research in it, it is not always cohesive or the best quality. I wanted to advance the profession in ways that make sense for physiotherapists, not in a silo of just research but in ways that are accessible to therapists, so that is why I went into research.”
What inspired you to integrate video games and virtual reality into your research?
“It was when I was doing my PhD when the Nintendo Wii first came out in 2007 and I was working with kids at the time. We thought we would start to integrate it, and we saw some of the benefits quickly, but also some of the disadvantages quickly. Benefits were mostly in terms of motivation, getting kids to do things that they might otherwise not do, or for longer. But then disadvantages were that it gives a lot of negative feedback, or kids were upset they weren’t performing as well as before their injury. I was always seeing that therapists were struggling to see the role it could play in their interventions. A lot of popular media at the time was coming out saying things like “Wii-Habilitation” and “maybe you don’t need the actual therapist, all you need is this video game console” and that felt very threatening to therapists. My work then was looking at how do we integrate it, how do we support therapists to make decisions about when to use it, when not to use it, how do we understand what goals to use it for, when should we stop, how do we measure whether it is effective? It was that console which was more video game than virtual reality that got me into it.
Then I moved on to different types of virtual reality. Now, especially in my role at the Technopole at Marie-Enfant, because we have so many different technologies, it is more in general about how do you and why would you choose a technology that could be complicated, could break, that you might not know how to use. How can we have enough evidence or rationale to ask therapists to change their practice to use those technologies and how can we do more than just buy the expensive piece of equipment and expect people to know what to do with it. It’s a lot about behavior change and knowledge translation.”
Next, we had the chance to briefly discuss a paper Dr. Levac published in 2019 called Performance Variability During Motor Learning of a New Balance Task in a Non-immersive Virtual Environment in Children with Hemiplegic Cerebral Palsy and Typically Developing peers [1]. This article discusses the variability in motor skill acquisition, retention, and transfer in children with cerebral palsy (CP) as compared to typically developing (TD) children using non-immersive virtual environments (VE). It was found that older children with CP had the least between-child variability in acquisition and the most in retention, while older TD children demonstrated the opposite pattern. These findings can inform further research investigating VE-specific causes of performance variability, including differing movement execution requirements and individual characteristics.*
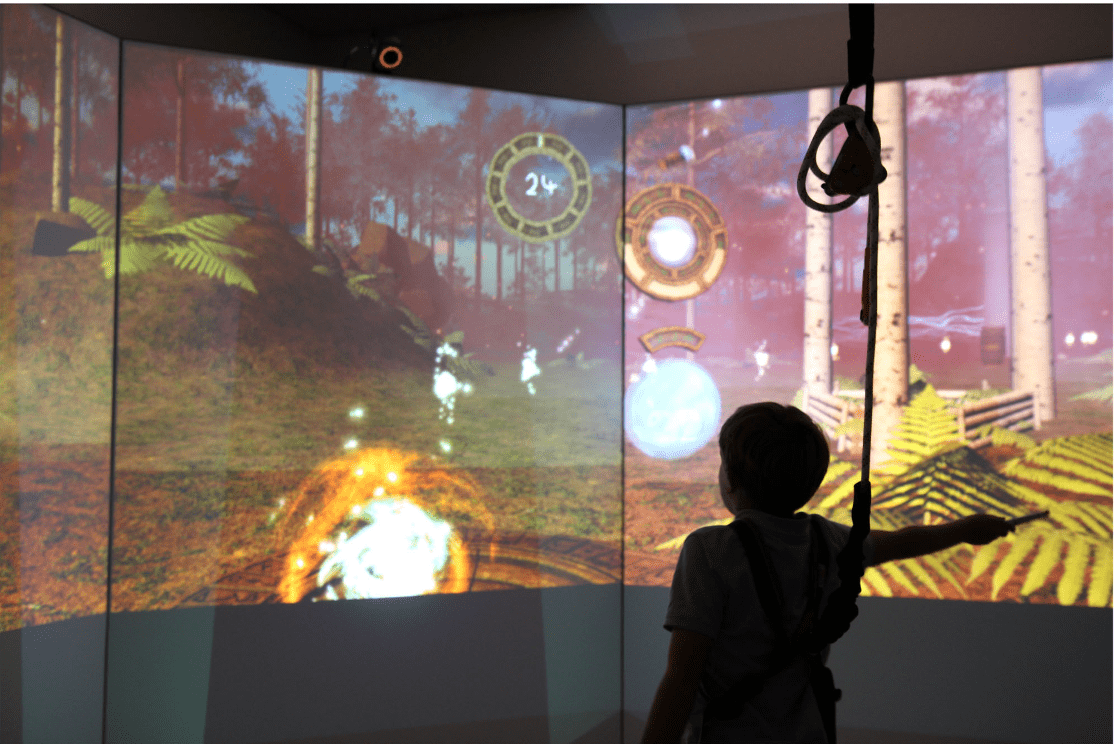
The image above is taken from the article in question, showing the non-immersive VE used in one of the studies. Children were tasked with moving their center of pressure to control a virtual avatar.
In this article variability is defined in different ways, some consider it detrimental, others a benefit. How would you define variability?
“The variability aspect is so interesting, there is this dichotomy. I think it’s how performance changes over time, within an individual or between individuals, that could be a result of development, skill acquisition or learning. At both those levels, they are really important things to research because we can’t find the signal of a treatment if everyone is so variable and so different within the group. Variability gets thrown out usually as an error or a mistake, but really that’s where we can learn a lot more about how to personalize a treatment, or what it might be about me that makes me react a certain way as opposed to another person. I think variability is an easy thing to dismiss as error or noise, and because it’s so complicated we tend to do that. But I think that’s where the interest and the meat of a lot of questions lies, especially in rehabilitation because no two clients are the same. If we can focus more on both how I change overtime and how my rate of change is different from yours and figure out why that might be, then we can better tailor our interventions to be more effective.”
What was your biggest takeaway from this study?
“The takeaway is there might be something about virtual reality because of two things. One, is that you might be a bit more variable in virtual reality than in the real world because, especially in non-immersive virtual reality, you’re reaching for things but they’re not actually there so, you don’t have that end contact of grabbing something. We should keep that in mind, if we’re training in virtual reality we should think, are we actually teaching people to do things in the same way as they would in the real world, so is virtual reality more variable? And second is to look more at variability over time and between people in your research to see if there is anything there that can tell you either why your intervention is effective or why you aren’t seeing a difference between your two conditions. Those might be my two takeaways. We used a method for quantifying variability that could be readily used in other studies, and we put the spotlight on variability where maybe it wasn’t before and maybe it leads others to think of variability as important or how they might consider it in their studies. The point of this study wasn’t to ask if the virtual environment was effective or did it work, but just to explore and see what we could learn from that data.”
Finally, we talked about the future of using technologies like immersive virtual environments in rehabilitation for children, including its advantages and limitations. One of the things about this line of research that Dr. Levac describes as both exciting and frustrating is the fact that the hardware and software is always changing. Unfortunately, the pace of technological development is much faster than clinical practice changes, and the rate knowledge is translated into practice. Dr. Levac notes that it is easy to be reactive when using these new technologies but stresses the importance of understanding the “key active ingredients” that might make them better (or worse) than other treatments. Many physiotherapists hesitate to integrate these technologies into practice, without being convinced it is safe and offers an added benefit, which is where Dr. Levac’s research comes in. Dr. Levac also highlights an important advantage of virtual reality, stating that it can equalize the playing ground between children with disabilities and their peers, giving them opportunities that wouldn’t otherwise exist. It can also bring you to environments that may otherwise be inaccessible or unreachable, offering social and equality potential benefits as well, once the cost barrier is overcome.
Can we expect virtual reality to become a regular part of physiotherapy?
“I think it will as long as costs continue to go down, and I think it’s something interesting therapists can offer. There’s also the potential to use it at home, so that’s a really good attractiveness for physiotherapists. Because of the interest factor, the motivation factor and the gaming factor the patient might be more likely to do it at home, because most people don’t do their exercises. So, the short answer is yes, but again it will only be in larger centers, that are more well-resourced, until the cost barriers can be reduced and we don’t need big computers to run it. Some technologies you don’t, like the Quest is already 500$ and you’re running. The problem is some of those games are accessible, others are not. A person with disabilities may have limitations when they interact with that technology, for example with the controllers it can be really hard to hold them after you have a stroke, if you don’t have any motor control in your hands. We need to see more accessible interaction methods and controllers, and that’s already coming.”
Though there is still some hesitation from clinicians and parents alike, there can be a lot of benefits as long as we continue to gain a better understanding of how it works, why it works and how to integrate into practice. It can make rehabilitation as exciting as your favourite video game, helping eliminate one of the biggest barriers physiotherapists encounter: keeping patients motivated to do their exercises. Dr. Levac explains:
“For most therapists, motivation is a big barrier, so if it’s something the client is interested in, and they are not afraid of it then they [physiotherapists] are willing to do a little bit of work to adapt it. And that’s why we need more rehabilitation games that are designed by engineers and clinicians together so that they aren’t just like the off the shelf games, but they include things that are important for rehab, movements that are important for rehab, and they measure things that are relevant. That’s where we can really gain is if we use low-cost hardware with rehab specific games.”
On a final note, virtual reality and other digital technologies offer the possibility of being innovative and promising rehabilitation tools, as long as research continues to answer many of the questions regarding how it works, why it works and how to use it effectively. It’s so exciting to see where this takes the field of rehabilitation, maybe in the future you will be playing video games as part of your physio exercises.
References:
[1] Cheng, M., Anderson, M., & Levac, D. E. (2021). Performance Variability During Motor Learning of a New Balance Task in a Non-immersive Virtual Environment in Children With Hemiplegic Cerebral Palsy and Typically Developing Peers. Frontiers in neurology, 12, 623200. https://doi.org/10.3389/fneur.2021.623200
*Part of this paragraph was written using OpenAI (artificial intelligence).